Last updated: Sat, Mar 22, 2025
If behaviorist analysis of pain relies on (observable) environmental conditions, or stimuli, and (observable) behaviors of subjects, what is the role of pain itself (subjective and not observable) in the analysis? Consider the basic model of behavior in the following diagram.
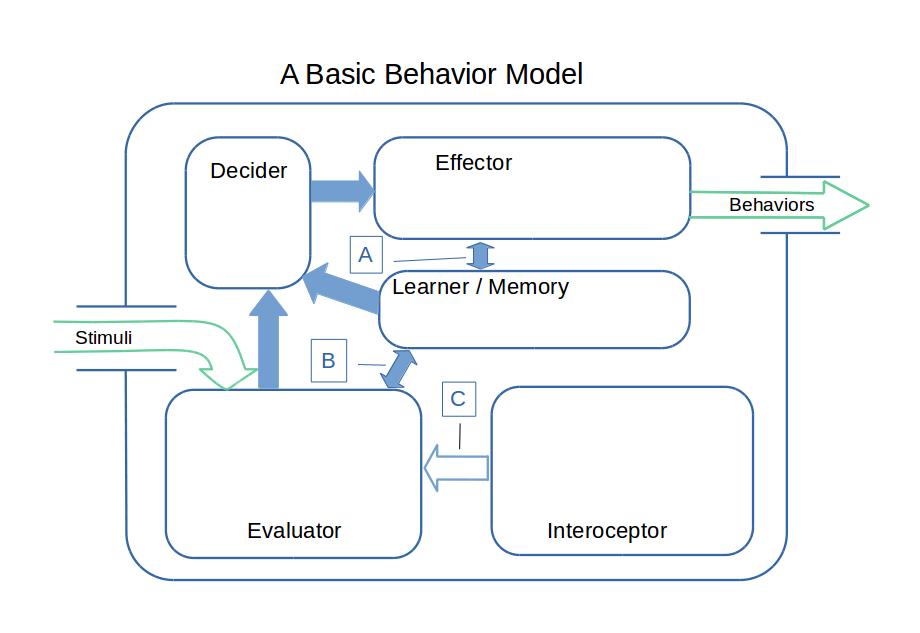
In the figure you see a large green arrow entering a box from the left with another large green arrow leaving the box on the right. These arrows represent the observable environmental conditions and the observable behaviors of an individual. The large box represents, in abstraction, the psychological processes that occur within the individual. This large box is labeled "A Basic Behavior Model."
Behavioral analysis is formally independent of unobservable psychological processes, yet learning theory calls for a minimal set of cognitive processes. These are represented by boxes within the large box. These represent logically necessary functions, not distinct areas of the CNS. The model ignores much complexity that we know complicates our minds.
Toward the center of the model is a function labeled "Learner/Memory." This function is needed to enable learning to occur. Its responsibilities include storing, retaining, and reporting what has been learned, and what is learned includes not only explicit memories but also what we might call "behavioral tendencies" or habits, and perhaps preferences as well. When behavioral learning occurs, it is stored away here and is then available to other cognitive processes.
In the bottom left of the model is another function labeled "Evaluator." Stimuli must be evaluated before they can trigger either behaviors or learning. This is the function of the Evaluator. As the model receives stimuli from the outer world, it must interpret them and must decide their significance. When the Evaluator is evaluating, it has access to what has been learned. This is indicated in the diagram by a blue arrow between the Learner/Memory function and the Evaluator function, which is labeled "B" in the diagram.
In the upper left is a function labeled "Decider." The Decider function decides on actions to be taken. It takes input from both the Evaluator and Learner/Memory, as indicated by the large blue arrows.
In the upper right is the function labeled "Effector." It brings into effect the stragegies that the Decider passes to it, and has access to the organisms learning, as indicated by the blue arrow labeled "A."
In the bottom right is a function labeled "Interoceptor." This module supplies information to the Evaluator about the state of the organism. The Interoceptor is the part of the process that is aware of pain, but it is aware of much more. The name "Interoceptor" is taken from "interoception," which includes all the aspects of the state of being that are perceivable to the organism. The scope of interoception includes all of the things that you can sense about yourself: your tension level, your tiredness, your happiness, the positions of your limbs and the orientation of your head, etc., etc.
Because the diagram shows a behaviorist model, the arrow ("C") in the figure, which feeds information from the Interoceptor into the Evaluator, is shown as hollow. Only stimuli and behaviors (shown in green) are observable.
In life, organisms (including ourselves) are continually evaluating stimuli, making action decisions, observing the consequences of their own actions, and learning as a result. In behaviorist thinking, learning occurs through the repetitive association of behaviors with consequences that are favorable. A fundamental chore for the Evaluator is to decide whether the consequences of the last behavior were positive or negative, rewarding or punishing.
The second figure shows the Basic Model, but only the learning phase of the ongoing process. The figure shows how the model learns after the organism has performed some behaviors and observed the consequences. The model has to evalute this feedback and learn from it. Only the Evaluator, Learner/Memory and Interoceptor are involved. In behaviorist learning, feedback that is rewarding (positive) causes learning that increases the likelihood of the behavior, while feedback that is aversive (negative) causes learning that decreases the likelihood that the behavior will be repeated under similar circumstances.
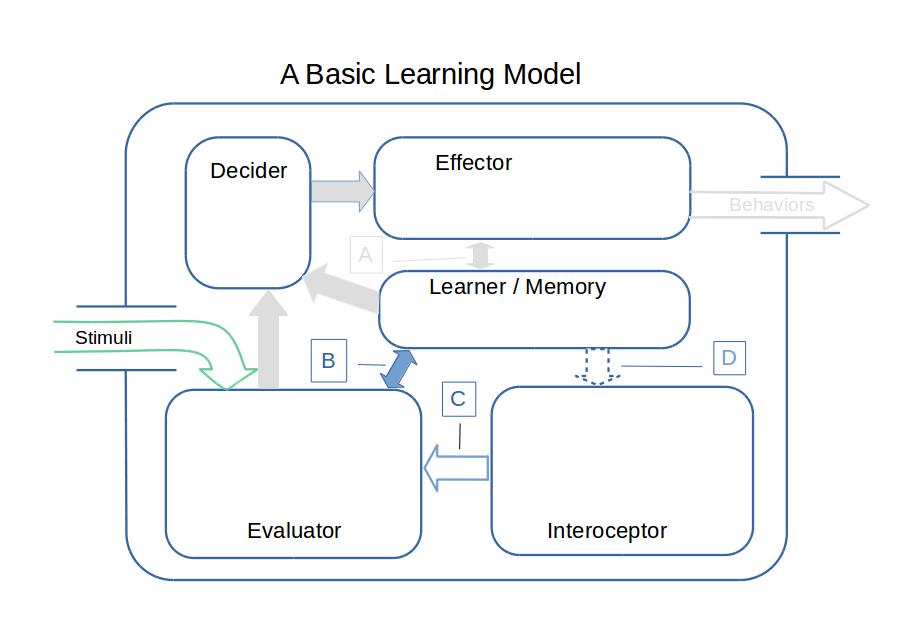
Arrow B, which connects Learner/Memory to the Evaluator, is two-way. The decision of the Evaluator, whether the feedback is positive or negative, travels from the Evaluator to Learner/Memory. Learned information/preferences can travel from Learner/Memory into the Evaluator. This allows prior learning to affect the evaluation.
Arrow C leads from the Interoceptor to the Evaluator. It reports interoceptive information to the Evaluator so that it can inform the Evaluator's decision. Arrow C can carry pain information, and it can also carry information about stress levels, moods, and the state of the limbic system. (See Motive, Behavior, and Learning and related sections.)
Arrow D has been added to the diagram. If Arrow D carries information, it carries memories or tendencies or preferences that modify the contents of Arrow C. That is, Arrow D allows for learning to modify the organism's interoceptions.
The innards of this model are not observable to clinicians. They can't observe the flows through the various arrows, nor the subject's interoceptive state. Nor can they read the learning that has accumulated within Learner/Memory.
They can only observe (imperfectly) the stimuli that the subject has received, and the behaviors that the subject performs. The organism's provides only dim and noisy clues to the learning process. Perhaps the subject smiles or sighs. Perhaps the subject grimaces or shifts position. These clues are ambiguous at best, as explained in Pain Measurement. Whether a smile or grimace is related to the evaluation of feedback or to something entirely different is unknown.
There is, however, substantial science that supports the existence of Arrows B, C, and D. Consider, for example, post-traumatic stress. PTSD exists, in the terms of this model, in Learner/Memory. It is accepted that PTSD triggers can cause changes to the interoceptive readings, Arrow C. During an episode, stimuli that are otherwise neutral or pleasant can be quite aversive. Stimuli as inherently innocuous as images or odors can change the state of the body and thus the reading of the Interoceptor.
Attempting to modify the pain behaviors of a patient is justified if the behaviors are indeed maladaptive and if it is possible to modify those behaviors in such a way that benefits outweigh costs. The clinician who wishes to diagnose behavior as learned and maladaptive is thus in a tenuous situation. Mechanisms for learning pain behaviors are known to exist. Pain behaviors can be maladaptive if the pain has changed but the behaviors haven't, or arguably because they were maladaptive when they were learned. However, it isn't possible to know either the extent to which the behavior is learned, nor to know whether the behavior is maladaptive.
The psychologically-oriented therapist can observe the subject's environment and behavior but can only surmise the subject's motivations. The therapist can collect biographical data and make inferences about past learning based on that data. They can accept the subject's report that changes in mood preceded changes in pain and infer causality, but such inferences can neither be proven nor disproven.
It is notable that many of the behaviors that have been proposed as products of maladaptive learning can be directly explained as adaptive responses to the existence of painful conditions. Concern over pain could be catastrophizing. Inactivity could be learned helplessness. Fear of pain may not be necessary and prudent, but maladaptive.
The effects of pain on the subject can't be known to observers because they occur within the black box that is the subject. Many known effects of severe and persistent pain aren't salient to external observers because our empathetic sense is derived from our personal experiences, and most people never experience life as a chronic pain sufferer. (Mirror Neurons and Empathy.) Training is a weak tool to compensate for this, because there is little research or training about aspects of pain other than pain intensity. The categorization of these effects as co-morbidities means that they tend to be the concern of a different specialty than that of the current care provider. (Co-morbidities.) Problematic sleep, high sympathetic tone, and other effects tend to be addressed by specialists who know little about their causal link to pain.
This confluence of factors provides a favorable environment for care providers to see the complaints through their personal lenses. The judgment that a behavior is maladaptive is always made based on preferred theories. This can put into question the nature of the pain that the subject complains of. The IASP pain definition clearly accepts that the subject's pain may not be a direct result of conditions in the body of the subject, and leaves it up to the treatment provider or the researcher to "accept" or not the reports of the subject.
These factors also lead to the use of "exaggerated," "maladaptive," "catastrophizing," and so on to describe behaviors. However, what is truly exaggerated or maladaptive depends upon the interoceptive reading of the subject, the type of learning that has in fact occured, and other factors that are obscure to the clinician. Many of the factors that have been proposed as learned causes of pain complaints are easy to criticize, as I report in The CBT Model of Pain and Pain Behavior and An Evaluation of CBT Theories of Pain. The hypothesis of "learned pain" always seems plausible under a behariorist lense because no possible observations of the subject are able to negate the hypothesis.
The basic premise of cognitive-behavioral therapy for pain is that corrected cognitions can result in alleviation of suffering. Doubtless there are incorrect cognitions that lead to increased suffering, and which can be corrected cognitively. How much of pain conditioning, though, can be altered cognitively? (Evidence for Pain Conditioning.) Much of pain conditioning isn't based on "cognition" as it is generally understood.
Consider the reorganization of somatosensory cortex that accompanies extended pain. (The Pain Matrix in Chronic Pain States.) This reorganization results in increased pain. It occurs without the awareness of the sufferer, quite automatically, yet it is considered "implicit learning" or "conditioning" in behavioral psychological terms. It can be corrected by relieving the conditions that caused it, whether that is some persistent pain generator or some form of neuropathy. It is a far stretch to construe such forms of relief as "cognitive."
This is not to say that there is any dearth of mistaken beliefs and appraisals encountered in the rehabilitation of chronic pain. Where these exist they should be dealt with cognitively. However, it is a grave error with serious consequences to exaggerate the potential role of CBT in pain management. It should be seen as an adjunct to the work of medical and manual therapists and not over-promised. There is often a thin line separating cognitive-behavioral therapy from simple behavioral counter-conditioning.
In medical parlance, "clinical" means treatment as it is practiced. How does this behavioral model work in practice?
Clinicians, whether they are pain doctors, psychologists, psychiatrists, physical therapists, or chiropractors, are subject to the same limitations as are researchers. They can't read your pain, your learning, or your memories. They can observe your environment while in the clinic, and they can observe your behavior in the clinic. They can ask you about your own introspections. The conditions within your psyche are not visible to them. When clinicians make judgements about your pain behaviors, they can only do so based on a lot of inference. There is no reliable test that is able to distinguish between exaggerated behaviors and appropriate behaviors. There is no reliable test to distinguish catastrophizing from appropiate concern. There is no reliable test to distinguish pain behaviors from other behaviors.
The judgements of clinicians will be highly influenced by their general beliefs about human nature. (Human Nature.) Psychologists will prefer psychological explanations, manual therapists will prefer biomechanical explanations, medical doctors will have varying views. Such analyses share many features with ideological understandings, where the truth or falsity of a proposition is judged by its congruence with the ideology.
There is a high risk of two kinds of errors. One is the error of identifying adaptive behavior as maladaptive. (Call this Type I.) The other is the error of identifying maladaptive behavior as adaptive. (Call this Type II.)
First consider the Type I error, in which adaptive behavior has been identified as maladaptive. What are the consequences for the subject?
Perhaps the subject will be encouraged to undergo some version of CBT therapy in an attempt to replace the adaptive behavior with some replacement behavior which, by assumption, is less effective. Or perhaps the clinician will attempt to change behavior less openly by hinting, nudging, and asking leading questions.
Suppose that the replacement behavior is mildly less effective than the subject's original behavior. In this case the subject may accept and practice the replacement behavior. The subject may report improvement in their overall condition, but this may be the result of placebo effects and/or regression to the mean. In this case, we would expect the reported improvement to extinguish over time and the subject's original behavior to resume. Precisely this pattern has been reported of CBT-based therapies. (See An Evaluation of CBT Theories of Pain.)
Suppose instead that the replacement behavior is much less effective than the subject's original behavior. In this case the subject may resist the therapist's efforts to change their behavior. In this case, I would expect that the clinician who recommended the behavior change might well interpret this behavior of the subject as also maladaptive. Remember that, just as there is no objective evidence to prove the clinician's opinion, so there is no objective evidence to refute it. The subject may be seen as responsible, then, for the continuation of their own suffering.
In either case, what is the cost to the subject? The time and money may be the least of it. In either case, the subject may have replaced a more-effective behavior with a less-effective one. To the extent that the subject sees the clinician as all-knowing, they will question their own judgement and accept the clinician's analysis, at a time when there are susbstantial demands on the subject to adapt to a new role in life. (The Challenge of Living in Pain.)
There is no good reason to suppose that the existence of the behavioral analysis affects only the clinician and the subject. It may affect other professional and non-professional caregivers, as well as makers of medical policy and research-funding decision makers. This would lead to shorting the search for root causes of the pain.
Next consider the Type II error, in which maladaptive behavior has been accepted by the clinician as adaptive or benign. What are the consequences for the subject?
In this case, the maladaptive behavior continues. Treatment continues along non-psychological lines, assuming the suffering is severe. The costs in time, money, and procedure-caused suffering to the subject are known to the subject and are borne by the subject. The costs that are paid by third-party payers are closely tracked, and treatments that are ineffective are discouraged by means of restrictions on delivery that are embodied in Medical Necessity Guidelines.
It seems likely that in practice many clinical assessments of behavioral pain will be mistaken, with serious consequences for sufferers and wasted resources throughout the medical research and medical treatment systems. Based on this analysis, I would suggest several actions:
If behavioral diagnoses were based on objective measurements, it would be possible to estimate the frequency of Type I and Type II errors. If the consequences of each type of error were known, medical protocols would be modified to minimize the costs of these errors. Such an analysis is routine in making medical policy, but it is not possible in this case. The subjective (not observable) nature of suffering is one factor here. (But see What's Better?.) Another factor is the "subjective" nature of the diagnosis. Here, "subjective" means "based not solely on objective observations and analytical reasoning, but influenced by the a priori beliefs of the diagnostician."